|
Health Benefits |
Silver |
Gold |
Platinum |
|
Extended Health (coverage per person) |
|||
|
Health Practitioners |
$250 combined |
$350 combined |
$400 per specialist per year |
|
Hospital (Preferred Wards) |
Unlimited |
Unlimited |
Unlimited |
|
Ambulance Services |
$1,500 |
Unlimited |
Unlimited |
|
Air Ambulance |
Unlimited |
Unlimited |
Unlimited |
|
Accidental Injury to Natural Teeth |
$2,000 per injury |
$2,000 per injury |
$2,000 per injury |
|
Private Duty Nursing |
$2,500 |
$2,500 |
$5,000 |
|
Breast Prosthesis |
1 for lateral / 2 for bilateral per 2 years, per person |
1 for lateral / 2 for bilateral per 2 years, per person |
1 for lateral / 2 for bilateral per 2 years, per person |
|
Wheelchairs, Scooters |
$500 per 5 years |
$500 per 5 years |
$500 per 5 years |
|
Patient Walkers |
$200 per 3 years |
$200 per 3 years |
$200 per 3 years |
|
Casts and Crutches |
Unlimited |
Unlimited |
Unlimited |
|
Artificial Eyes,
|
$10,000 lifetime max. |
$10,000 lifetime max. |
$10,000 lifetime max. |
|
Diabetic Supplies
|
$300 |
$300 |
$500 |
|
Ostomy Supplies |
$300 |
$300 |
$300 |
|
Oxygen Equipment |
$500 |
$500 |
$500 |
|
Out-of-Province Referral |
n/a |
$50,000 lifetime |
$50,000 lifetime |
|
Custom Foot Orthotics |
1 pair every 5 years (adult) /1 pair per year for children under 17 yrs. |
1 pair every 5 years(adult) /1 pair per year for children under 17 yrs. |
1 pair every 5 years (adult) /1 pair per year for children under 17 yrs. |
|
Therapeutic Shoes |
n/a |
$200 |
$200 |
|
Hearing Aids |
n/a |
$500 per 5 years |
$500 per 3 years |
|
Blood Pressure Monitor |
n/a |
n/a |
1 per policy per 5 years |
|
Additional Expenses |
$500 combined |
$500 combined |
$500 combined |
| Survivor Benefit | 12 month | 12 months | 12 months |
|
Travel |
|||
|
30 days (unlimited number of trips) |
n/a |
$5 million total coverage |
$5 million total coverage |
|
Vision Care (coverage per person) |
|||
|
Eye Exams, Glasses |
$60 per 2 years |
$150 per 2 years |
$300 per 2 years |
|
Prescription Drugs (coverage per person per policy year) |
|||
|
Coverage
Pay-direct Card included with all options |
70% of cost up to $1,000 |
80% of cost up to $3,000 |
100% of cost to $5,000 |
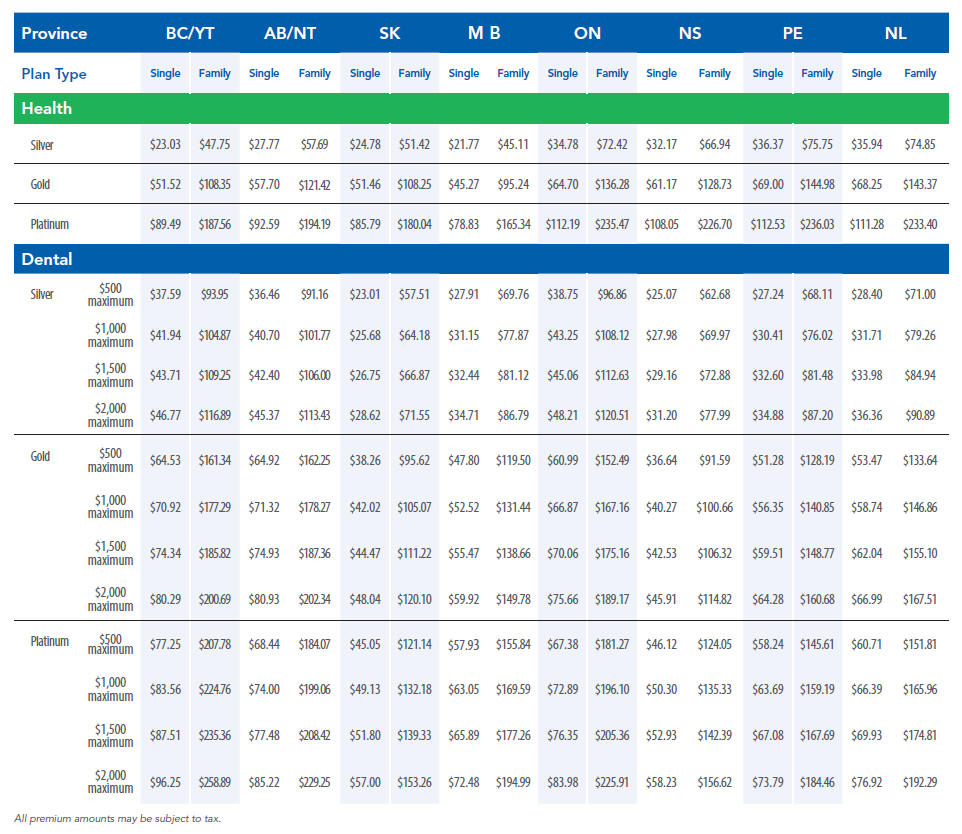
GMS Group Advantage Dental Benefits at a Glance
Dental plans include employer choice of $500, $1,000, $1,500, or $2,000 combined annual coverage maximum
for basic and major services, per person, per year.
|
Dental Benefits |
Silver (3+ employees) |
Gold (3+ employees) |
Platinum (6+ employees) |
| Co-insurance | Co-insurance | Co-insurance | |
| Preventive Services | 80% | 100% | 100% |
| Basic Services | 80% | 100% | 100% |
| Major Services | n/a | 50% | 80% |
|
Orthodontic Services |
n/a | n/a |
50% |
Dental Services